Vitrectomy
What is Vitrectomy?
Vitreous is a transparent, gel-like texture that fills the inside of the eyeball. It covers about two-thirds of the eye volume and contributes to the formation of the anatomical shape of the eye. In diseases of the posterior segment of the eye, vitrectomy surgery, that is, vitreous gel may require surgical evacuation. After vitrectomy, vitreous gel is replaced with an intraocular secretory fluid called humor aqueous.
Vitrectomy, or Pars Plana Vitrectomy (PPV), is a partial or complete discharge of the transparent gel, ie vitreous, that fills the wide space in the back of the eye by entering into the eye with a cutting and absorbent device with a diameter of less than 0.5-1 mm. The emptying of the vitreous allows the vitreoretinal surgeon to reach the retina and the pathologies that occur in it.
Vitrectomy, or Pars Plana Vitrectomy (PPV), is a partial or complete discharge of the transparent gel, ie vitreous, that fills the wide space in the back of the eye by entering into the eye with a cutting and absorbent device with a diameter of less than 0.5-1 mm. The emptying of the vitreous allows the vitreoretinal surgeon to reach the retina and the pathologies that occur in it.
What is the purpose of vitrectomy?
In these surgeries, it is aimed to clear the bleeding, withdrawal bands, intraocular foreign body or infection in the intraocular fluid (vitreous) and to restore the retina (neural network layer) to the old anatomical structure. If bleeding, inflammation cells, foreign bodies and scar tissues disrupt the visual function by preventing the image from reaching the perceived retina, this should be corrected by vitrectomy. If vitrectomy is not treated, blindness and total loss of the eye may occur. For example, if a patient with retinal tear, detachment, intraocular infection, and foreign body is left untreated, loss of light sensation and physis may be unavoidable over time. The primary purpose of surgery is to prevent such situations. Generally,first vitrectomy surgery is planned to achieve anatomical and visual success; sometimes, repeated operations may be necessary to achieve this.
Vitrectomy in which eye diseases?
There are many reasons for vitrectomy. The most important indications:
- Diabetic retinopathy (advanced pathologies in diabetes)
- Vitreous hemorrhage (intraocular hemorrhage)
- Macular hole (hole in the center of vision)
- Macular pucker (wrinkle in the center of vision)
- Retinal detachment and ruptures (rupture of the eye’s nerve network layer)
- Pretetinal membranes (membranes formed in the neural network)
- ROP (in premature retinopathy that can be seen in infants staying in the oxygen tent for a long time due to preterm delivery)
- Complications of lens residue in the eye after cataract surgery
- Endophthalmitis (Intraocular infections after cataract and other eye surgery)
- Treatment of eye injuries and intraocular foreign body removal
How is vitrectomy performed?
Vitrectomy can be performed under local or general anesthesia.
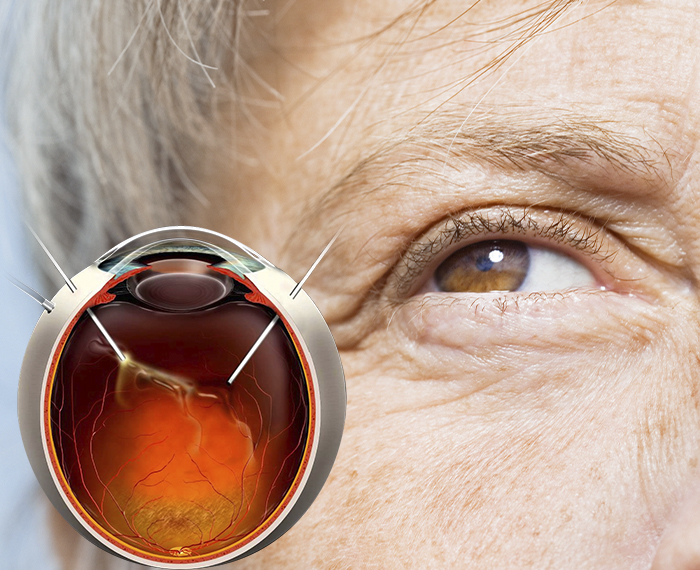
When the eye is viewed from the front of the colored (iris (in front of the iris layer that gives the eye color), which looks like a round, transparent watch glass, the white part of the sclera outside the area called aladuran cornea is made by micro-incision (usually close to the color part called Pars Plana). one is used to deliver fluid to regulate intraocular pressure, the other inputs are used for the source of light for image purposes, and the input of the vitrector device.
Vitrectomy surgeries are performed with the help of advanced technology vitrectomy device developed for this purpose by using contact lenses or noncontact imaging systems, laser device (to stick the retinal tear) in order to see the inside of the patient under the operating microscope. Depending on the type or severity of the disease in your eye, air, gas, silicone tampon materials may be required instead of liquid. Air or silicone continues the treatment of the disease in your eye after the surgery, as long as it stays in the eye. These materials may include silicone recovery. Others, ie air and gas, are absorbed from themselves. However, air / gas in the eye during this period (up to 1 week) (up to 2 months for gases) reduces the patient’s vision;in silicone oil users, the eye starts to see from the first day, but the eye is less visible – until the silicone oil is removed. In recent years, trans conjunctival vitrectomy systems (in which the operation can be completed without suture application) have been used and seamless operations have been performed with very small entrances with minimal side effects.
When the eye is viewed from the front of the colored (iris (in front of the iris layer that gives the eye color), which looks like a round, transparent watch glass, the white part of the sclera outside the area called aladuran cornea is made by micro-incision (usually close to the color part called Pars Plana). one is used to deliver fluid to regulate intraocular pressure, the other inputs are used for the source of light for image purposes, and the input of the vitrector device.
Vitrectomy surgeries are performed with the help of advanced technology vitrectomy device developed for this purpose by using contact lenses or noncontact imaging systems, laser device (to stick the retinal tear) in order to see the inside of the patient under the operating microscope. Depending on the type or severity of the disease in your eye, air, gas, silicone tampon materials may be required instead of liquid. Air or silicone continues the treatment of the disease in your eye after the surgery, as long as it stays in the eye. These materials may include silicone recovery. Others, ie air and gas, are absorbed from themselves. However, air / gas in the eye during this period (up to 1 week) (up to 2 months for gases) reduces the patient’s vision;in silicone oil users, the eye starts to see from the first day, but the eye is less visible – until the silicone oil is removed. In recent years, trans conjunctival vitrectomy systems (in which the operation can be completed without suture application) have been used and seamless operations have been performed with very small entrances with minimal side effects.
What are the problems in vitrectomy?
In cases where air / gas is given into the eye, it may be necessary to lie face down for days (3 days-3 weeks). Intraocular pressure may increase early in the postoperative period and may block the retina’s nourishing vessel to achieve complete blindness. Common side effects of the surgery are the acceleration of cataract development, the possibility of re-bleeding, and the retina (network layer) to be removed. In such cases, re-surgery may be required.
When is Visual Recovery Improved after Vitrectomy?
Vitrectomy is the most difficult operation for ophthalmologists to predict postoperative vision. If there is any systemic (such as sugar and hypertension) or eye disease affecting the vitreous and retina, various treatments such as drugs or lasers are applied, but if the disease progression cannot be stopped, vitrectomy is performed. Unfortunately, artificial intraocular retina has not been produced with the technology reached by the current medical science. As a result, retinal tissue that is damaged during surgery, previously laser, needles or trauma is tried to be repaired. In other words, tissue replacement is performed by vitrectomy surgery, not tissue replacement. The anatomical success of the surgery is to achieve these goals, functional success,in other words, the level of vision that can be obtained in the retina (network layer), which has nerve tissue and cannot be regenerated, can only be determined after a certain period of time. Of course, these results are related to the extent to which the sensitive structures that provide vision were affected before the operation. If the previous damage is small, the increase in visual acuity is very high and if the effect is very high, the visual level increases.
What should patients pay attention to after vitrectomy?
- After surgery, the eye should remain closed until the first check unless otherwise stated. (You can get clean closure cotton and strips from the pharmacy and change them daily)
- The eye should not touch the water for a week (unless otherwise stated); the head should be washed from the back and the body should be washed separately so that water does not get into the eyes. The eye should be thoroughly cleaned with wet cotton. After a week, you can take a shower with the eye closed and without scrubbing.
- Eye wipes, paper towels etc. not clean. should not be deleted with.
- No pressure should be applied to the eye.
- It should be informed from the doctor which drugs should be used while being discharged, how many times a day and how long it should be instilled.
- After discharge, some stinging and pain in the eye (responsive to painkillers) may be considered normal.
- It is essential that the physician obtain information about whether a substance has been introduced into the eye (such as air, gas, silicone). After the operation, the head position is important and you should ask the doctor how to lie down and how long you should lie down and stay in that position.
- If intraocular vitrectomy gas is given, it is normal to have a black darkness in front of the eye. Depending on the type of intraocular gas, it will remain in the eye for 2-6 weeks and it is normal for it to stop seeing during this period. It is forbidden to travel by plane to patients who are given gas!
- Other travel means should be preferred until the gas is fully withdrawn; This period may last between 2 weeks and 2 months after surgery according to the nature of the gas given. If general anesthesia is needed for any reason (in case of emergency), the anesthesiologist should be informed that there is gas in the eye and appropriate anesthetic substance selection should be provided accordingly. There is a small risk of retinal detachment or bleeding recurrence after the gas has been withdrawn. Therefore, inspection examinations should not be limited.
- If silicone oil is given into the eye, it is usually left in the eye for 3-6 months and then a new surgery is performed to remove it. Since silicone is likely to deteriorate after a while and cause eye damage (redness of the eye, increased eye pressure, etc.), it is absolutely necessary to check it periodically. It should also be kept in mind that retinal detachment after silicone removal has a risk of recurrence.
- If you have new or progressive pain in the operated eye (not responding to painkillers), increased redness, sudden or progressive worsening of vision level, you should be evaluated by your physician who performs the surgery as soon as possible, or by an ophthalmologist near you.